(June 17th, 2026) Webinar: Doppler-Derived Hemodynamics to Assess Cardiac Remodeling in Mice with Transverse Aortic Constriction
(June 17th, 2026) Webinar: Doppler-Derived Hemodynamics to Assess Cardiac Remodeling in Mice with
This webinar will address topics ranging from validating surgical outcomes to tracking disease advancement, encompassing typical carotid and stenotic jet velocities, evaluations of cardiac function, coronary flow reserve, and cerebral perfusion through ophthalmic artery flow. If you’re new to TAC or seeking to enhance your monitoring methods, the session provides practical guidance for achieving more consistent and thorough cardiovascular outcomes.
Key Points:
Accurate, non-invasive physiological monitoring is key to reproducible animal research. Introduced over three decades ago, the cardiac pressure overload mouse model created by transverse aortic constriction (TAC) has undergone several procedural modifications. Regardless of the type of TAC procedure, it is crucial to confirm surgical success early, noninvasively monitor the outcomes, and to stratify the animals based on severity of stenosis. Measurements typically include Doppler flow velocity, along with structural imaging by ultrasound or MRI. This presentation will focus mainly on the Doppler measurements that include the standard left and right carotid flow velocities, stenotic jet velocity, and aortic and mitral velocities to study cardiac function. Furthermore, coronary flow reserve which defines the heart’s functional capacity to increase blood flow when oxygen demand rises and the potential to measure cerebral perfusion via left and right ophthalmic artery flow velocities during TAC will be discussed.
Topics discussed in this webinar include:
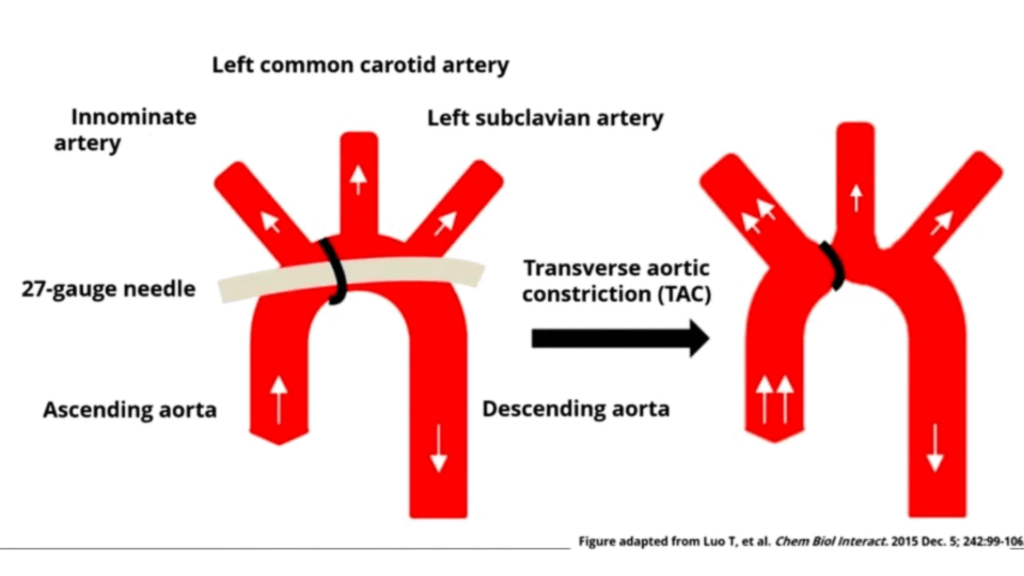
Transverse Aortic Constriction (TAC) is a challenging surgical procedure developed to study the cellular and molecular pathways of left ventricular cardiac hypertrophy and heart failure. Since its introduction over three decades ago, TAC has undergone several modifications. Key advancements include the shift from highly invasive open-chest surgeries to minimally invasive closed-chest procedures; this transition minimizes inflammatory responses and the complex physiological compensations required to maintain stability at both the systemic and cellular levels.
Originally, TAC utilized silk or nylon sutures, which often caused variability in stenosis size or suture slippage. While O-rings with fixed inner diameters were introduced to ensure consistency, they can create artifacts during echocardiographic imaging. Furthermore, imprecise O-ring placement can lead to inconsistent pressure gradients, damage to surrounding structures, or unintended lung congestion caused by pressure on the pulmonary artery. Other specialized methods include “de-banding” (removing the constriction) to study reverse remodeling.
Studies: Mouse TAC models simulate human pressure-overload conditions, such as aortic stenosis or hypertension. By surgically narrowing the aortic arch between the brachiocephalic trunk and the left carotid artery, chronic pressure overload is induced. The heart follows a predictable timeline – a) 1-2 weeks of early compensatory phase when the heart adapts via concentric hypertrophy (wall thickening) to maintain function. This often results in a temporary preservation or enhancement of cardiac contractility. b) 4-8 weeks of decompensated phase when the heart progresses into left ventricular (LV) dilation as it can no longer compensate for the pressure.
A big advantage of Doppler measurements is that they can be made immediately after ligation of the aorta before closing the skin to confirm the success of TAC. Additionally, Doppler measurements can be made at several time points during studies lasting 8-12 weeks providing multiple snapshots of the disease progression. This allows researchers to monitor gradual changes and to evaluate the precise timing of drug therapies or de-banding effects.
Regardless of the specific TAC technique used, it is vital to confirm surgical success early and noninvasively monitor outcomes to stratify animals by stenosis severity. While measurements include structural imaging via ultrasound or MRI, this presentation focuses primarily on Doppler measurements. These include standard left and right carotid flow velocities, stenotic jet velocity, and aortic and mitral velocities. Additionally, we will discuss the status of coronary flow reserve – which defines the heart’s capacity to increase blood flow under oxygen demand – and the distribution of ophthalmic artery blood flow as a potential index of cerebral perfusion during TAC.
*Note: The topic discussed will exclusive be on Doppler applications in TAC.

Anilkumar Reddy, PhD, is a Principal Scientist at Indus Instruments, where he leads preclinical product development and the exploration of novel biomedical applications. During his extensive career at Baylor College of Medicine, he specialized in evaluating cardiac and vascular mechanics in rodent models to advance methods for the early detection of cardiovascular diseases that included atherosclerosis, aortic stenosis, and myocardial infarction, hypertension, and others. Dr. Reddy has championed the use of non-invasive methods, such as pulsed Doppler flow velocity and ultrasound imaging, to phenotype animals and monitor cardiovascular adaptations during disease progression. At Indus, he contributes to the design, development, and testing of custom sensors and instrumentation used to assess physiological and cardiovascular function in small animals.
(June 17th, 2026) Webinar: Doppler-Derived Hemodynamics to Assess Cardiac Remodeling in Mice with
(June 11th, 2026) Webinar: Overview of Small Animal Cancer Models and Imaging Applications
(April 9th, 2026) Webinar: Driving NAMs-Aligned Preclinical Research with the Newton 7.0 Optical
(March 12, 2026) Webinar: Preclinical Imaging of Multiple Myeloma Bone Disease by Dual-Energy
(February 25, 2026) Webinar: How to Optimize Your Western Blot Workflow and Choose
(February 12, 2026) Webinar: Sharper Images, Stronger Studies- Optimizing Your Preclinical Ultrasound Techniques