System Used:
NGB-R

Maxime Abellan Lopez1,2* Laurence Hutter3 Etienne Pagin3 Mélanie Vélier2,4 Julie Véran2,4 Laurent Giraudo2,4 Chloe Dumoulin2,4 Laurent Arnaud5 Nicolas Macagno6 Romain Appay6 Laurent Daniel6 Benjamin Guillet2,7 \Laure Balasse2 Hugo Caso1 Dominique Casanova1,2 Baptiste Bertrand1,2 Françoise Dignat2,4 Loïc Hermant3 Hélène Riesterer3 Fabien Guillemot3 Florence Sabatier2,4 Jérémy Magalon2,4
- 1Plastic Surgery Department, Hôpital de la Conception, AP-HM, Marseille, France
- 2Aix-Marseille Université, INSERM, Institut National de Recherche Pour l’Agriculture, l’Alimentation et l’Environnement, Centre de Recherche en Cardiovasculaire et Nutrition (C2VN), Marseille, France
- 3Poietis, Pessac, France
- 4Cell Therapy Department, Hôpital de la Conception, AP-HM, INSERM CIC BT 1409, Marseille, France
- 5Vascular Biology Department, Hôpital de la Timone, AP-HM, Marseille, France
- 6Anatomy and Pathology Department, INSERM U1263, C2VN, Hôpital de la Timone, Marseille, France
- 7Centre Européen de Recherche en Imagerie Médicale (CERIMED), Aix-Marseille Université, Centre National de la Recherche Scientifique, Marseille, France
Introduction: An autologous split-thickness skin graft (STSG) is a standard treatment for coverage of full-thickness skin defects. However, this technique has two major drawbacks: the use of general anesthesia for skin harvesting and scar sequelae on the donor site. In order to reduce morbidity associated with STSG harvesting, researchers have developed autologous dermo-epidermal substitutes (DESs) using cell culture, tissue engineering, and, more recently, bioprinting approaches. This study assessed the manufacturing reliability and in vivo efficacy of a large-size good manufacturing practice (GMP)-compatible bio-printed human DES, named Poieskin®, for acute wound healing treatment.
Methods: Two batches (40 cm2 each) of Poieskin® were produced, and their reliability and homogeneity were assessed using histological scoring. Immunosuppressed mice received either samples of Poieskin® (n = 8) or human STSG (n = 8) immediately after longitudinal acute full-thickness excision of size 1 × 1.5 cm, applied on the skeletal muscle plane. The engraftment rate was assessed through standardized photographs on day 16 of the follow-up. Moreover, wound contraction, superficial vascularization, and local inflammation were evaluated via standardized photographs, laser Doppler imaging, and PET imaging, respectively. Histological analysis was finally performed after euthanasia.
Results: Histological scoring reached 75% ± 8% and 73% ± 12%, respectively, displaying a robust and homogeneous construct. Engraftment was comparable for both groups: 91.8% (SD = 0.1152) for the Poieskin® group versus 100% (SD = 0) for the human STSG group. We did not record differences in either graft perfusion, PET imaging, or histological scoring on day 16.
Conclusion: Poieskin® presents consistent bioengineering manufacturing characteristics to treat full-thickness cutaneous defects as an alternative to STSG in clinical applications. Manufacturing of Poieskin® is reliable and homogeneous, leading to a clinically satisfying rate of graft take compared to the reference human STSG in a mouse model. These results encourage the use of Poieskin® in phase I clinical trials as its manufacturing procedure is compatible with pharmaceutical guidelines.
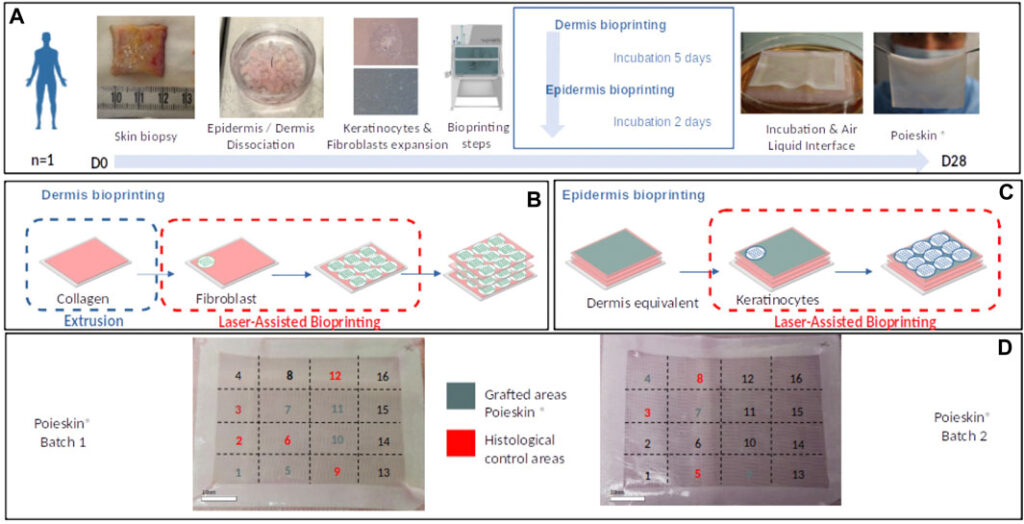
FIGURE 1. (A) Summary of main Poieskin® manufacturing steps. (B) Dermis bioprinting steps: successive bioprinting of collagen layers with extrusion bioprinting and fibroblast layers with laser-assisted bioprinting (LAB). (C) Epidermis bioprinting steps: keratinocyte deposition with LAB. (D) Final repartition of Poieskin® product batches 1 and 2 between histological control and grafts on mice

FIGURE 2. Study design comparing human split-thickness skin graft (HSTSG) to Poieskin® (OR, operating room).
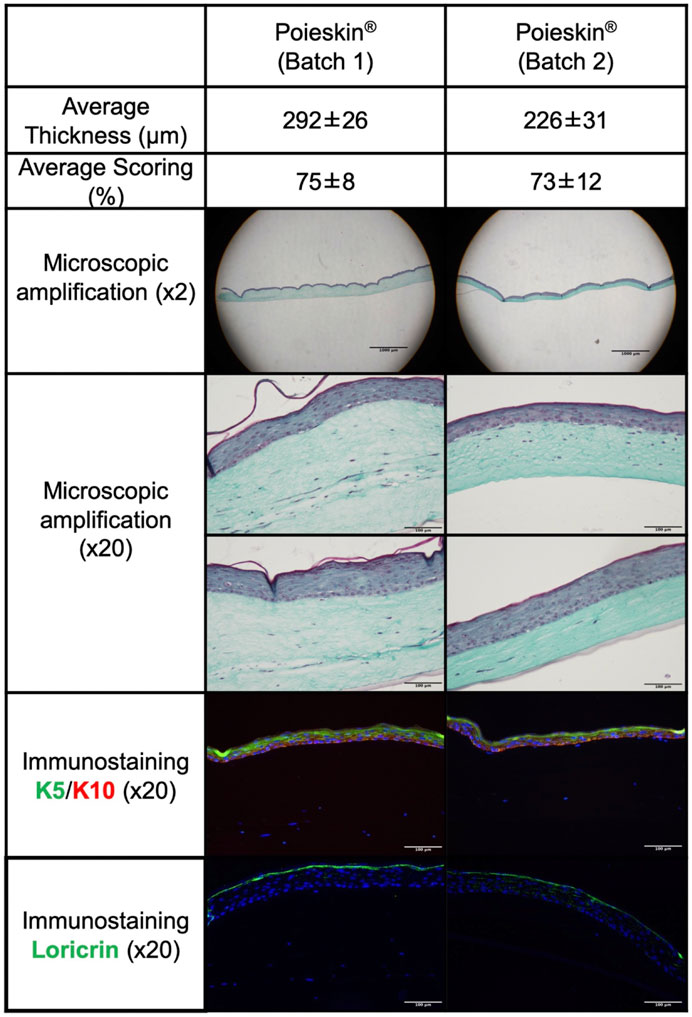
FIGURE 3. Histological and immunostaining characterization of Poieskin® manufacturing: Poieskin® batch 1: area 6 control of mouse 2, scoring = 78, and thickness = 355 ± 33 μm; Poieskin® batch 2: area 3 control of mouse 6, scoring = 81, and thickness = 219 ± 45 µm.

FIGURE 4. Grafted area measurements on standardized photographs ((A) Photograph of grafted Poieskin® on day 0; (B) photograph of grafted Poieskin® on day 16 with contouring of the total scarring area; (C) photograph of grafted Poieskin® on day 16 with contouring of the graft lysed area; (D) assessment of graft take; (E) assessment of graft retraction; HSTSG, human split-thickness skin graft).
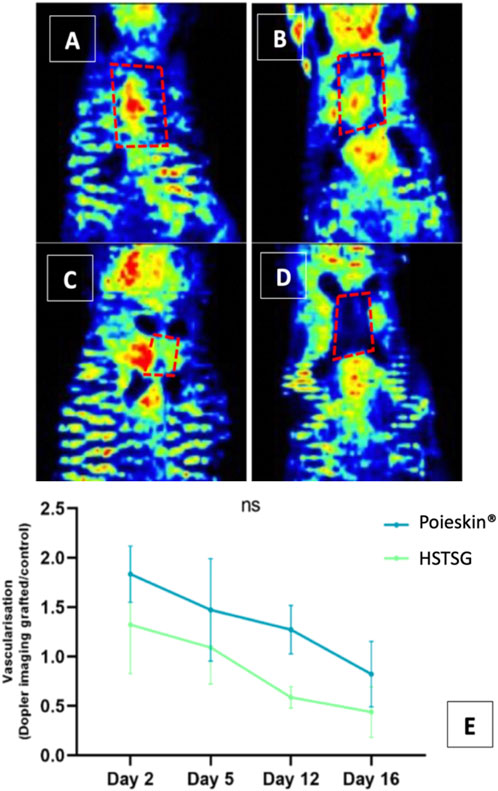
FIGURE 5. Graft perfusion assessment by laser Doppler ((A) Poieskin® condition on day 2; (B) HSTSG condition on day 2; (C) Poieskin® condition on day 16; (D) HSTSG condition on day 16; (E) evolution of the optical density ratio for both conditions).
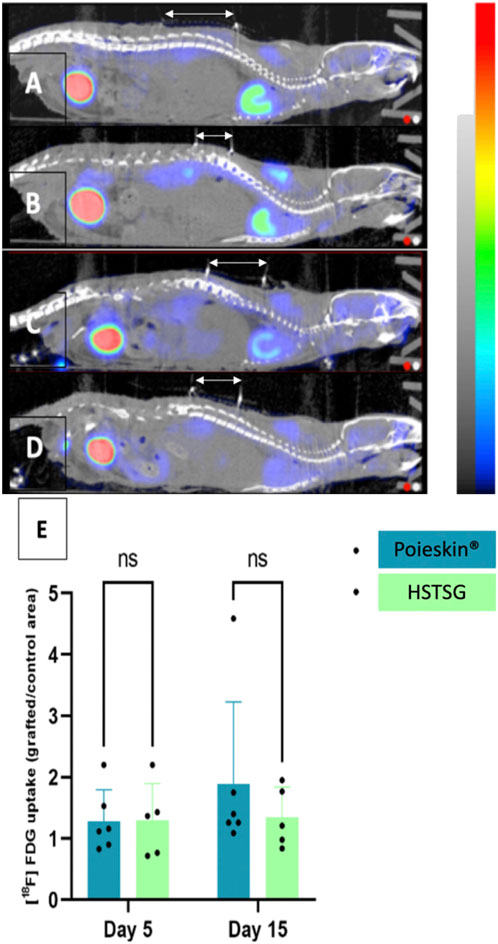
FIGURE 6. [18F]-FDG MicroPET/CT imaging (CT signal from −500 to 3,500 HU; PET signal from 0 to 8 Bq) 1 h after IV injection. Grafts are located below the white arrows ((A) Poieskin® on day 5; (B) HSTSG on day 5; (C) Poieskin® on day 15; (D) HSTSG on day 15; (E) metabolic activity measurements).
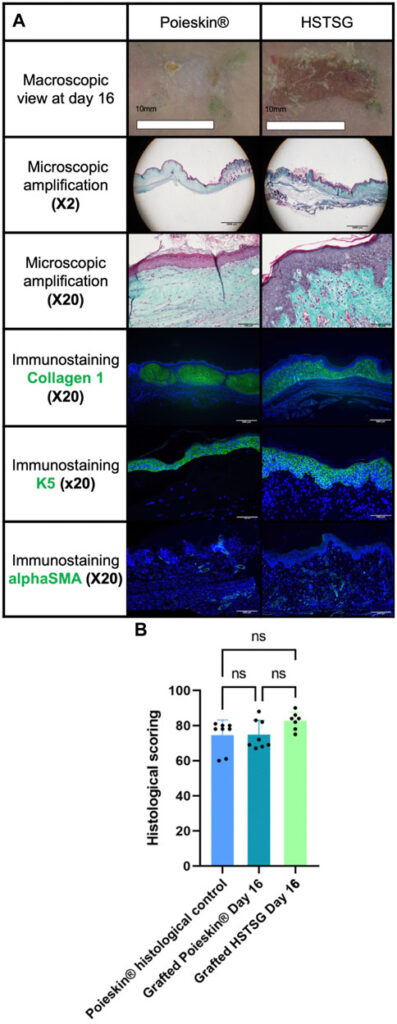
FIGURE 7. Results of histological analysis. (A) Representative images of the histological aspects of Poieskin® (mouse 8, batch 2, area 9, scoring = 69, and thickness >300 µm) and human split-thickness skin graft (HSTSG) (mouse 9, scoring 84, and thickness >300 µm); (B) exhaustive results of histological scoring for Poieskin® control, grafted Poieskin®, and grafted HSTSG.