Article review: “Effects of Isoflurane on Coronary Blood Flow Velocity in Young, Old, and ApoE−/− Mice Measured by Doppler Ultrasound”
System Used:
Prospect T1
The heart needs to constantly adapt to changing metabolic conditions and physiological stressors, such as exercising and aging. Within that same principle, coronary arteries that supply the heart with blood to maintain normal cardiac functioning must adapt, mainly by changing arterial vessel dimensions and subsequent blood flow to the heart. For example, when exercising, the heart needs increased blood flow to itself or cardiomyocyte ischemia can occur1. This maximal blood flow to the heart is called coronary flow reserve (CFR). When needed, this protective mechanism allows the heart to respond to increased blood demand by increasing the blood flow, called a hyperemic state.
Coronary flow is notoriously difficult to measure so many researchers have opted for implantable probes and catheters. However, coronary disease can also be hidden under baseline conditions in many pathological models and is only uncovered when the heart is under demand, shown through the hyperemic state2. For example, the resting flow of a narrowed coronary artery does not always change, but when demand on the heart is added, maximal blood flow through this narrowed artery and thus CFR is significantly reduced, showing clear underlying pathology3. Induction of a hyperemic state of a blood vessel requires another step, and researchers typically choose between challenging the animal with exercise or hypoxia or administering a vasodilator, like adenosine, usually through intravenous infusion or an osmotic pump4,5. With the vasodilator adenosine specifically, in a normal coronary artery, this results in approximately a fourfold increase in flow rate compared to baseline6. Although all of these techniques are effective for CFR analysis, they are very labor-intensive and are invasive research procedures, complicating longitudinal studies.
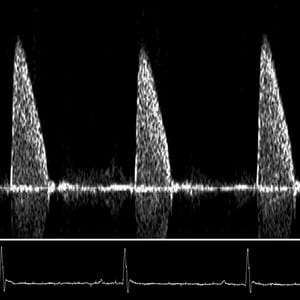
A paper published in Ultrasound in Medicine and Biology by researchers from the Baylor College of Medicine and The Methodist Hospital showed a simplified technique that acquires CFR in mice using a common anesthetic with secondary dose-dependent vasodilator properties, Isoflurane7. Using the Doppler Flow Velocity System, the researchers measured coronary flow velocity at both a hyperemic and a baseline state. They stimulated hyperemic conditions by increasing the concentration of isoflurane gas to 2.5% and for baseline conditions isoflurane gas was lowered to 1%. This technique allows future researchers to test CFR reliably, longitudinally, and quickly. Since this is a non-invasive procedure using Doppler, this can easily be added to longitudinal studies to check if there may be narrowing, blockage, or bulging of the coronary arteries in multiple pathological models. Figure 1 shows representative baseline and hyperemic coronary doppler signals from a two-year-old WT mouse and a two-year-old ApoE−/− mouse. At both baseline and hyperemic states, the ApoE−/− have increased velocity, indicative of coronary lesions, which is likely in this atherosclerosis-prone model. Recently, these coronary flow reserve measurements made by Doppler technology have been established as feasible and accurate8–13. This current research and others have shown the niche research applications that Doppler technology can extend to, especially in simplifying complex protocols.
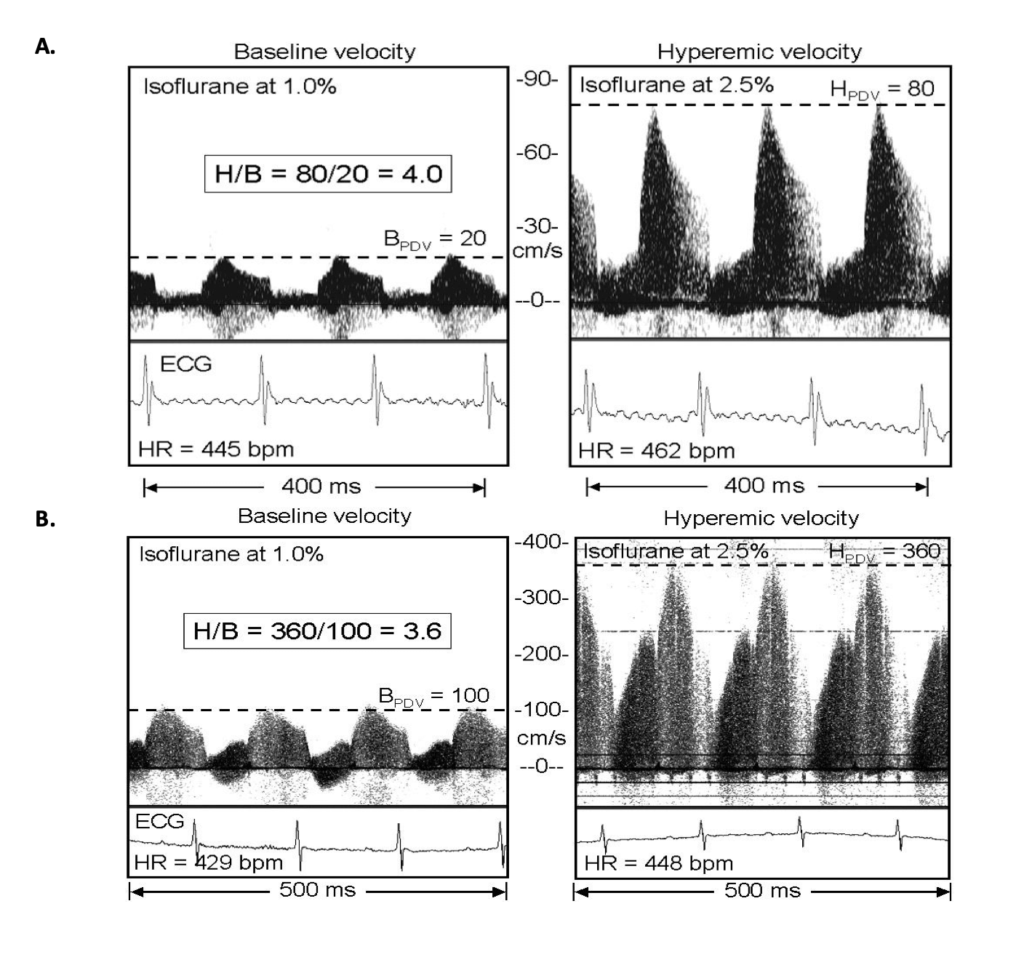
Figure 1: Coronary Doppler signals from A. an Old WT mouse and B. an ApoE−/− mouse with presumed stenosis (estimated to be 75% by area) of the left main coronary artery. Baseline velocity was taken at low (1%), and hyperemic velocity was taken at high (2.5%) levels of isoflurane gas. The horizontal lines show the average peak diastolic velocity (PDV) at baseline or during hyperemia in each panel. (*Figures from Hartley, C. J. et al. Ultrasound Med Biol vol. 33 (2007).
References
1. Rahman, H. et al. Coronary Microvascular Dysfunction Is Associated With Myocardial Ischemia and Abnormal Coronary Perfusion During Exercise. Circulation 140, 1805–1816 (2019).
2. Shantouf, R. S. & Mehra, A. Coronary fractional flow reserve. American Journal of Roentgenology vol. 204 W261–W265 (2015).
3. Gould, K. L. & Lipscomb, K. Effects of coronary stenoses on coronary flow reserve and resistance. The American Journal of Cardiology 34, 48–55 (1974).
4. Gould, K. L., Lipscomb, K. & Hamilton, G. W. Physiologic basis for assessing critical coronary stenosis: Instantaneous flow response and regional distribution during coronary hyperemia as measures of coronary flow reserve. American Journal of Cardiology 33, 87–94 (1974).
5. Wikström, J., Grönros, J., Bergström, G. & Gan, L. M. Functional and morphologic imaging of coronary atherosclerosis in living mice using high-resolution color Doppler echocardiography and ultrasound biomicroscopy. Journal of the American College of Cardiology 46, 720–727 (2005).
6. Bicycle exercise stress in PET for assessment of coronary flow reserve: repeatability and comparison with adenosine stress – PubMed. https://pubmed.ncbi.nlm.nih.gov/12571202/.
7. Hartley, C. J. et al. Effects of Isoflurane on Coronary Blood Flow Velocity in Young, Old, and ApoE −/− Mice Measured by Doppler Ultrasound. Ultrasound Med Biol vol. 33 (2007).
8. Hozumi, T. et al. Noninvasive assessment of coronary flow velocity and coronary flow velocity reserve in the left anterior descending coronary artery by Doppler echocardiography: comparison with invasive technique. Journal of the American College of Cardiology 32, 1251–1259 (1998).
9. Caiati, C., Zedda, N., Montaldo, C., Montisci, R. & Iliceto, S. Contrast-enhanced transthoracic second harmonic echo Doppler with adenosine: a noninvasive, rapid and effective method for coronary flow reserve assessment. Journal of the American College of Cardiology 34, 122–130 (1999).
10. Voci, P. et al. Measurement of coronary flow reserve in the anterior and posterior descending coronary arteries by transthoracic Doppler ultrasound. The American journal of cardiology 90, 988–991 (2002).
11. Pizzuto, F. et al. Assessment of flow velocity reserve by transthoracic Doppler echocardiography and venous adenosine infusion before and after left anterior descending coronary artery stenting. Journal of the American College of Cardiology 38, 155–162 (2001).
12. Voci, P., Pizzuto, F. & Romeo, F. Coronary flow: a new asset for the echo lab? European heart journal 25, 1867–1879. (2004).
13. Trifunovic, D. et al. Usefulness of coronary flow reserve measured by transthoracic coronary Doppler ultrasound in. the elderly. Journal of Geriatric Cardiology : JGC 14, 436 (2017).